What
are the underlying differences between contortionists
and others - at the molecular or genetic level?
The
answer is not known.
There
was an early view in the medical profession, from
Beighton, Grahame and others, that contortion arises from collagen
disease.
That is, they suggest that contortion is a variant of the Joint
Hypermobility
Syndromes such as Marfan Syndrome and Ehlers-Danlos Syndrome. These
arise from
mutations in the genes coding for collagen and related molecules.
Others
suggest that some aspects of this view are wrong.
Patients with collagen diseases have weak collagen, and tend to suffer
from a
large number of disabilities, with fragile tissues, often including
ruptured
blood vessels, heart and intestinal problems, frequent dislocation of
the
joints, and joint pain. In addition, those studied by Beighton, Grahame
and
associates initially presented at the clinic with pathological symptoms
(joint
dislocations, joint pain, tissue damage) so the conclusions may be based
on a
sample already selected for pathology.
In
contrast, contortionists tend to be very strong and fit,
although they are also very stretchy. Their collagen is strong, not
fragile.
While laxity may mean that contortionists tend to dislocate their
joints
relatively easily, with training they are able to strengthen and
protect those
joints so that in a contortion act they can perform incredible feats of
strength (such as a one-hand handstand, holding an inverted position
for a long
time, or holding the weight of the lower body over the head in an
extreme
backbend, requiring great strength in the lower spine). Performing contortionists
do not
in general suffer the problems of tissue fragility seen in Ehlers-Danlos and similar Syndromes.
Therefore
it might seem that Ehlers-Danlos Syndrome
and contortion ability are quite separate phenomena, presumably with
different
molecular bases. However, while we do not know the molecular bases of
many of
these diseases, or of ability in contortion, there is an emerging view
that all
hypermobility syndromes, benign or not, may be related, and may be part
of the same
spectrum of phenomena, though with different outcomes in different
individuals
(reference 1). Moreover, some performing contortionists go on to
develop clear signs of Ehlers-Danlos Syndrome later in life (in Ehlers-Danlos Syndrome, hypermobility tends to dominate early in life, while other symptoms tend to dominate later in life). This suggests that in such individuals extreme flexibility and Ehlers-Danlos syndrome are related.
One hypothesis is that
flexibility
with strong collagen, such as can be found in
contortionists, could be related to the degree of crimp in collagen.
Collagen
gives flexible tissues strength, and under a microscope it has a wavy
structure
(called “crimp”). When collagen is stretched, the waviness gets
straightened out,
so the collagen stretches easily at first. Once the waviness has got
fully stretched out, the stiffness of the collagen increases markedly.
It is
likely
that variations in the degree of crimp, and how the collagen molecules
are
packed together, are able to affect the stretchiness of collagen while
keeping
it strong.
The
crimp appears to be derived from the basic molecular
structure of collagen and how the collagen molecules are packed (see
references
2-4) – variation in the related genes may be responsible for conferring
the
ability. A PDF file of a basic talk on some of these issues can be
found here
(the talk as presented included movies - not part of this PDF -
including those of the vertebrae moving; it also did
not include the more recent views described in reference 1).
There is evidence that the ability can be inherited. People in families with flexible family members often refer to which family members have or have not inherited “the bendy gene”. Early training is also important, but should not start too early because young and vulnerable bodies need to be protected, and strength, body awareness and control have to be trained along with flexibility. One trainer of young people has suggested that 25% of the population have the ability if training is started early.
For safety, it is important that not only strength, body awareness, stability, and control are trained along with flexibility, but that the individual should be only trained within the range that is appropriate for them. ”Traditional” methods and those used in environments where there is only a small respect for the integrity of the individual, can lead to damage which asserts itself more-or-less rapidly (e.g. after only a few years performing, and almost certainly in later life). One example of successful safe contortion is shown by Christine Danton (Christina Shillaker) who at the age of 70 was still performing her backbending contortion act, with only a small decrease in flexibility over the years. This is because she has always taken care of her own training and stayed within the range that is appropriate for her.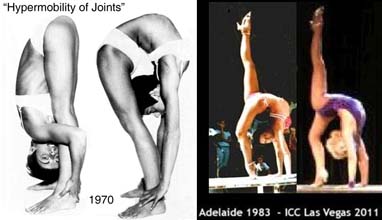
An
MRI study of contortionists by Peoples et al (2008) showed that
contortionists
could stay remarkably healthy and appear relatively youthful at least
up to the
age of 49 (the oldest measured in that study): “Given the degree of
stress
placed upon the spine by these elite athletes there was a surprisingly
limited
amount of pathological change present within their spinal column. This
no doubt
reflects their rigorous and dedicated training routines.” (5). These
subjects
were all Mongolian, and may have been exposed to relatively severe (and
hence
possibly damaging) traditional training in their early lives.
References:
Overview
of relation between different Joint Hypermobility
Syndromes:
1.
Castori
M, Colombi M. (2015) Generalized
joint
hypermobility, joint hypermobility syndrome and Ehlers-Danlos syndrome,
hypermobility type. Am. J. Med. Gen. C 169C: 1-5.
The
crimp in collagen, and the factors that affect
it:
2.
Miller KS, Connizzo BK, Feeney E, Soslowsky LJ.
(2012) Characterizing local collagen fiber re-alignment and crimp
behaviour
throughout mechanical testing in a mature mouse supraspinatus tendon
model. J.
Biomech., 45: 2061-2065.
4.
Franchi M, Raspanti M, Dell'Orbo C, Quaranta M,
De Pasquale V, Ottani V, Ruggeri A (2008) Different crimp patterns in
collagen
fibrils relate to the subfibrillar arrangement. Connect Tissue Res. 49:
85-91.
An
MRI study of contortionists: